
Psychiatry at the Margins
The Philosophical Foundations of HiTOP
A new paper examines the assumptions behind a new way of classifying mental illness
Mar 13, 2026
If you follow developments in psychiatric classification, you’ve likely heard of the Hierarchical Taxonomy of Psychopathology, or HiTOP. It’s one of the most ambitious attempts in recent decades to redescribe and reorganize mental health problems, moving away from the clinically familiar syndromic categories of the DSM and ICD toward a statistically driven framework that generates symptom profiles for patients along an array of dimensions. But what are the theoretical assumptions that underpin this project? What philosophical commitments does it carry, even when it presents itself as guided by data?
In a newly published paper led by me and co-authored with folks from the HiTOP Revisions Workgroup, we take on these questions directly. “Examining the Foundational Assumptions of the Hierarchical Taxonomy of Psychopathology” in Philosophy, Psychiatry, & Psychology offers a structured overview of the framework’s conceptual and philosophical underpinnings, while being mindful that these are matters of active debate, and there is expected to be disagreement among the consortium on many of these issues.
I have to say, working on this paper was an intellectual treat for me, and conversations and exchanges among the authors forced me to consider these issues with a conceptual rigor that deepened my own understanding of psychiatric classification in the process. I could not have asked for a better team of authors. It was a privilege for me to collaborate with people whose work I’ve previously read and admired, such as Aidan Wright, Miri Forbes, Eiko Fried, Chris Hopwood, and Bob Krueger. Colin DeYoung in the senior author role was a wonderful intellectual guide.
In this blog post, I want to offer an overview of the discussion and walk through the key themes of the paper in a manner that also touches on their significance for anyone interested in questions of classification and psychopathology. I also hope this post serves as encouragement for you to read the full article!
I do want to note that this paper is not an introduction to HiTOP. If you know almost nothing about HiTOP, you may want to start with a primer, e.g. this 2019 clinical introduction to HiTOP, this 2021 scientific overview of HiTOP, or my 2024 paper on diagnostic pluralism.
This paper was published as a “Philosophical Case Conference,” which means it is accompanied by 5 commentaries from authors across psychiatry, psychology, and philosophy (thank you Dost Öngür, Sam Fellowes, Brian Hood, Miriam Solomon, and Nick Zautra), and our response. The commentaries have also been published online ahead of print, but our response is still pending publication, so I will have more to say about the commentaries later.
Why HiTOP exists
To understand HiTOP, you first have to understand what it’s reacting to. Traditional diagnostic systems (that is, the DSM and ICD) organize mental illness into distinct categories: you either have “major depressive disorder” or you don’t; you either meet criteria for “generalized anxiety disorder” or you don’t. These systems were built on clinical tradition, expert consensus, and assume that mental disorders are best described as polythetic categories (meaning a checklist of criteria, a certain number of which must be met and various combinations are possible), regardless of how statistically coherent these categories are.
The trouble is that decades of research have exposed serious problems with this approach. Comorbidity is rampant. Patients routinely meet criteria for multiple disorders at once, far more than expected by chance, which raises the issue of whether these are truly distinct conditions or we are just slicing complex symptom profiles into clinically convenient but etiologically misleading pieces. Due to lumping together of variable presentations within any single diagnosis, patients can look strikingly different from one another (the heterogeneity problem). And the boundaries between “disorder” and “no disorder” are often arbitrary, with no clear natural threshold separating the two in the diagnostic manuals.
HiTOP consortium was launched in 2015 to address these shortcomings. It proposes organizing psychopathology as a hierarchy of dimensions, ranging from narrow symptom components and traits at the base to broad spectra (such as internalizing, externalizing, and thought disorder) at higher levels, all the way up to a general psychopathology factor (the “p factor”) at the top. The structure is derived from patterns of statistical covariation (essentially, which symptoms tend to go together in statistical analyses) rather than from clinical observation or theoretical tradition.
What does the HiTOP model actually represent?
This is the well-known (I hope) figure representing the current version of HiTOP:
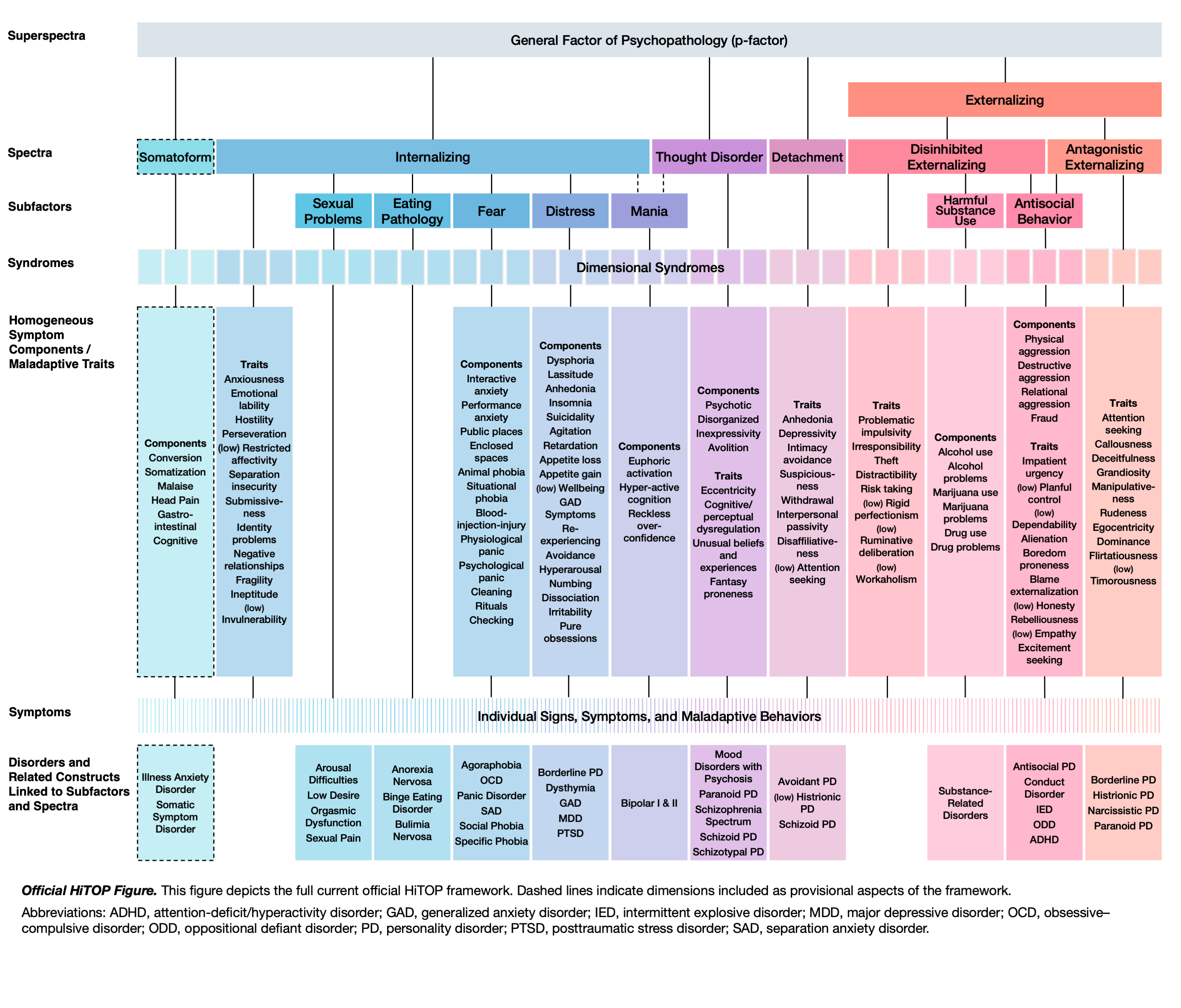
One of the first things our paper clarifies is what the official HiTOP model is and isn’t. It is not a fitted statistical model or a particular instance of it. Rather, the visual diagram is best understood as a heuristic, an expository scaffolding that represents patterns of covariation hierarchically without specifying exact mathematical values. It synthesizes a great deal of evidence from factor-analytic and related statistical studies, but the model itself is a conceptual summary.
The HiTOP model is fundamentally descriptive. It tells us how symptoms and traits cluster together, not why (at least for now). It is not etiologically guided; it does not claim to reveal the causes or mechanisms behind any particular cluster of symptoms. The hope is that getting the description right will ultimately facilitate better causal research, much as Linnaeus’s taxonomy of organisms provided a descriptive foundation that eventually paved the way for evolutionary theory. But that’s an aspiration, not a claim already realized.
The consortium relies primarily on quantitative evidence, with the stated aim of minimizing decisions driven by special interests, ideological traditions, or sociopolitical influences. The model also acknowledges uncertainty: constructs with limited evidence are flagged as preliminary, and the revision process is designed to be systematic and transparent. And as our paper emphasizes, “data-driven” does not mean “free from assumptions and values.”
HiTOP is not “atheoretical”
HiTOP has been described as a “quantitative nosology based on consensus of evidence,” which can easily be read as a claim that it is purely empirical or atheoretical. Our paper pushes back against this reading. The reality is that HiTOP relies on several significant assumptions.
The most obvious are the commitments to dimensionality and hierarchical organization: the ideas that psychopathology is best understood as continuously distributed in a population and that this variation is best organized in a nested, hierarchical structure.
The dimensionality assumption is based on taxometric evidence, hence, it is not an assumption in a deeper, foundational sense. If taxometric and other scientific evidence points out the existence of discrete categories, HiTOP will follow that evidence.
Three different meanings of “dimension” have been described in psychopathology literature. The first simply refers to continuous variables where indicators can be summed or averaged rather than used categorically, such as counting depression symptoms on a continuous scale (eg, Patient Health Questionnaire-9) rather than making a binary diagnosis. The second, more restrictive meaning requires that these indicators cohere statistically, fitting a unidimensional factor model where a single superordinate construct explains their covariance. The third and most restrictive meaning adds the requirement that the dimension be empirically distinguishable from related constructs within a multidimensional framework. HiTOP uses “dimensions” in this third most restrictive meaning, exemplifying a statistically coherent, multidimensional framework.
The hierarchy assumption is more fundamental. Although hierarchical models can statistically fit the data well, many alternative statistical models could potentially fit the same data. The assumption that clinical symptom clusters should be arranged within a hierarchy is untestable using only statistical data on covariance, but can potentially be supported with other forms of scientific evidence, such as associations with biomarkers at different levels of the hierarchy.
Beyond these two explicit assumptions, there are also theoretical considerations that are implicit. The reliance on factor analysis brings its own set of mathematical assumptions and biases. The historical decisions about what counts as “psychopathology” and what gets measured in the instruments whose data feed into the model shape the model’s scope in ways that aren’t always made visible.
From the perspective of philosophy of science, the idea that any scientific project could be entirely value-free or assumption-free is not tenable. All observation is theory-laden; all science operates within paradigms of shared assumptions, methods, and standards. HiTOP is no exception. Our paper draws on work in philosophy of science to frame scientific objectivity not as a “view from nowhere” that perfectly mirrors an independent reality, but as something achieved through transparent methods, systematic evidence evaluation, and being open to critiques. HiTOP’s commitment to quantitative rigor and transparent procedures is itself a methodological choice, one molded by the judgment that earlier diagnostic systems relied too heavily on clinical consensus and pragmatic considerations at the expense of statistical coherence.
What counts as “psychopathology”?
What does HiTOP mean by “psychopathology”? The answer, our paper notes, is that HiTOP does not have an official working definition. The consortium has been focused on structural organization — on mapping the covariance of symptoms — rather than on defining what makes something psychopathological in the first place. In practice, HiTOP has implicitly assumed that psychopathology is whatever clinicians and researchers have studied under that label over the course of history.
Concepts of mental disorder and psychopathology are heterogeneous and historically contingent. The domain of what counts as a mental disorder has expanded considerably over time, and different philosophical accounts of mental disorder, e.g. Wakefield’s harmful dysfunction analysis, Boorse’s biostatistical theory, DSM’s folk-psychological approach, cybernetic accounts, etc., would draw the boundaries of pathology in different places and different ways. HiTOP’s core model describes patterns of symptom covariation, but covariation alone doesn’t tell us whether something is functional or dysfunctional, a manifestation of difference or disorder, adaptive or maladaptive.
In other words, HiTOP addresses only some components of the broader concept of mental disorder (which includes components like clinical significance, dysfunction, and harm). It maps the terrain of symptom co-occurrence but leaves open the questions of clinical significance, dysfunction, and harm, the very questions that any complete account of psychopathology has to eventually confront. The silence is a deliberate feature at the moment, and it means that HiTOP’s descriptive model will eventually need to be integrated with a theoretical account of what makes certain symptom patterns pathological.
Although HiTOP as a statistically informed model is agnostic regarding notions of psychopathology, it can be a source of inspiration and support for theories of psychopathology. For instance, the HiTOP model suggests a continuity between dimensions of personality (the Big Five) and dimensions of psychopathology (HiTOP spectra), and this alignment provides an opportunity for theories of psychopathology seeking to explain them in terms of shared mechanisms. For an example of such a theory of psychopathology, see the cybernetic theory of psychopathology by DeYoung and Krueger.
Making sense of latent variables
Latent variables are statistical constructs that emerge from factor analysis (and related statistical techniques) and form the backbone of HiTOP’s evidence base.
Psychologists sometimes talk about latent variables as if they are hidden entities lurking inside the person, “causing” the symptoms we observe. But mathematically, a latent variable is simply a representation of the shared variance among a set of observed indicators. It is a statistical summary, not a causal account. The arrows in a factor model diagram represent statistical associations, not causal pathways, much like regression coefficients describe associations without necessitating causation.
HiTOP aims to be agnostic about the ontological status of its latent variables. It does not assume that a factor like “internalizing” represents a single hidden cause or causal essence. The observed covariation among symptoms could arise from common causes, from mutual reinforcement among symptoms (mutualism, aka network model, is when symptoms feed into each other, e.g., worry leads to insomnia leads to fatigue leads to more worry), or from some combination of both. HiTOP’s latent variables can be understood as dispositions, tendencies to act or behave in certain ways, that don’t come packaged with a specific causal story.
In the “common cause” model, symptoms of, say, depression co-occur because they’re all driven by some underlying depressive liability. In a mutualist or network model, they co-occur because they causally influence each other. The covariation is real either way, and a factor model will capture it as latent variables.
This mathematical interpretation of latent variables also sidesteps the traditional realism/anti-realism debate in the philosophy of science in our view. If no unobservable causal entity is being posited, if latent variables are understood purely as representations of covariation patterns, then the question of whether they “really exist” as hidden causes doesn’t come up in the usual way. Our paper suggests, tentatively, that this stance may have affinities with structural realism: the view that what successful scientific theories capture about reality is mathematical structure and relational properties rather than unobservable entities.
Dimensions, categories, and thresholds
The dimensionality assumption is supported by large meta-analyses of taxometric research finding that dimensional models fit the evidence far better than categorical models. But dimensionality at the population level doesn’t rule out possible discontinuities at the individual level. Phase transitions between states of health and illness, for instance, are theoretically compatible with a continuous distribution of symptoms between individuals.
Then there’s the practical question of what to do about diagnostic thresholds. Clinical practice needs categories: we have to decide who receives treatment, who qualifies for services, who is counted in prevalence estimates. HiTOP doesn’t reject the use of categories. Dimensional scores can be converted to severity categories using standardized T-scores along any of HiTOP dimensions, with suggested benchmarks for mild, moderate, and severe presentations. Unlike DSM’s fixed thresholds at the syndromic level, these cut-points are intended to be flexible, context-dependent, and usable at any level of hierarchy.
One important finding our paper highlights is that the relationship between symptom severity and impairment across most domains of psychopathology appears to be linear so far, without obvious inflection points. Unlike, say, blood pressure or HbA1c, where exponential increases in health risk at certain thresholds help justify specific diagnostic cut-points. In the absence of such natural thresholds, the choice of where to draw the diagnostic line becomes, inescapably, a decision that reflects social and practical attitudes, allocation of available resources, and judgments about how to handle access to care and the risks of over-diagnosis and over-treatment.
How does HiTOP handle validity?
Diagnostic validity, the question of whether diagnostic constructs correspond to something real and meaningful, has been a central concern in psychiatry since Robins and Guze’s influential 1970 paper proposing criteria for validating psychiatric diagnoses and the subsequent expansion and refinement of this approach by Ken Kendler. The DSM tradition uses a set of external validators (family studies, biological markers, treatment response, and so on) to assess whether categories are picking out genuine syndromes.
HiTOP follows what has been described by Nick Zautra as a “structure-first psychometric validity” approach. The first and most critical step is structural validity: does the construct accurately capture the patterns of covariation observed in symptom data? This is evaluated through factor-analytic methods and related methods such as principal component analysis. Only after structural validity is established does HiTOP turn to external validators (the same kinds of criteria used in the DSM tradition) to assess whether the constructs relate meaningfully to things like family aggregation, biological markers, treatment response, and course of illness.
This is a notable point of convergence: despite HiTOP’s criticism of DSM-style categories, it borrows the DSM’s validators for evaluating external validity. It also continues to rely on expert curation but the focus of expert curation is on synthesis and interpretation of psychometric evidence as primary. Although the revision process prioritizes systematic evaluation of quantitative evidence by transparent criteria, decisions about what to include and how to interpret the evidence ultimately still depend on committees of specialists. The need for human judgment in synthesizing and interpreting evidence remains, similar to how it is across medicine and science.
Values, diversity, and the limits of “objectivity”
HiTOP is, like all science, not “value free.” The paper devotes considerable attention to the role of values in HiTOP, both epistemic values (like empirical adequacy, parsimony, internal consistency) and non-epistemic values (like equity, clinical utility, inclusivity). Epistemic values are of primary importance in the development of the HiTOP model and take precedence over non-epistemic values whenever there’s competition, but non-epistemic values are also present and play a role.
The consortium has explicitly committed to ensuring that the model has clinical utility and that it is applicable to diverse, underrepresented, and epistemically marginalized populations. This consortium has a workgroup devoted to this issue, and the paper discusses concrete examples of how sociocultural context can affect the meaning and measurement of symptoms. Addressing this requires methodological adjustments as well as the inclusion of diverse perspectives in the model’s development. The discussion on this issue aligns with philosophical approaches of standpoint epistemology and methodological objectivity, along the lines that perspectives from marginalized groups and the diversity of the scientific community can reveal biases and assumptions that may otherwise be invisible.
Conclusion
HiTOP is an important step forward in the scientific classification of mental health problems. A concerted and sustained effort to establish a descriptive framework for psychopathology, rooted in quantitative evidence. But, like any scientific project, it has theoretical assumptions, it has guiding values, and it exists in a certain historical context. It has a context of discovery and a context of justification.
Our paper elaborates on these assumptions and choices, allowing clinicians and researchers to better understand, investigate, and critique HiTOP’s approach. HiTOP on its own is limited in what it can accomplish; it is one approach to psychopathology among many, and diagnostic pluralism is currently both a clinical and scientific necessity. We hope it encourages more philosophical discussion of the framework, both inside and outside the consortium.
The article pdf is available online ahead of print in Philosophy, Psychiatry, & Psychology. As always, I welcome your thoughts and reactions.
P.S. This is my personal summary of the article, prepared with considerably less caution than what went into crafting the original, which reflects the collective, iterative effort and agreement of all the authors. I have tried to be faithful to the paper in this post, but if there are any significant discrepancies in the language used here and the language used in the published article, the journal article obviously takes precedence as the authoritative version.
See also:

Examining APA’s Proposed Redesign of the DSM
·
6. März

DSM Disorders Disappear in Statistical Clustering of Psychiatric Symptoms
·
9. März 2024
Psychiatric Diagnosis and the Endgame of Validity
·
25. Oktober 2025
Psychiatry at the Margins is a reader-supported publication. To receive new posts and support my work, consider becoming a subscriber.
Discussion about this post
DSM Disorders Disappear in Statistical Clustering of Psychiatric Symptoms
Mar 9, 2024•Awais Aftab

A differential diagnosis for the weird and the awkward
Dec 5, 2025•Awais Aftab
What Do We Owe the Insufferable?
When mental illness exhausts our emotional capacities
Jan 30•Awais Aftab

Ready for more?
© 2026 Awais Aftab · Privacy ∙ Terms ∙ Collection notice
Start your SubstackGet the app
Substack is the home for great culture














































































 My mother showed me how to work hard and both my sister and mother encourage me to be myself.
My mother showed me how to work hard and both my sister and mother encourage me to be myself.